???????????????Division of Cardio??lo?gy
Special Interests / Research Projec?ts??
?
Rheumatic heart disease
Rheumatic heart disease [RHD] remains a huge burden world-wide despite it being virtually eradicated in the first-world countries. Because it is seen in mostly middle and lower-income countries, it receives vastly less funding for research and development of new treatment modalities than other causes of valve disease. Our Division has a special interest in both the diagnosis and treatment of this condition. Current diagnostic criteria was challenged by a large-scale community-based study [Echo in Africa] and a new technique for using a balloon to dilate narrowed valves was developed in the Division.
Valvular diseases
Because of the large burden of valvular pathology in our referral base, we are one of the leading units for the evaluation and treatment of heart valve disease. Evaluation is performed with state-of-the-art echocardiography machines as well as cardiovascular magnetic resonance imaging. We offer a wide variety of valvular interventions, including one of the first units in the world to offer percutaneous [non-surgical] replacement of all 4 of the heart's valves, non-surgical closure of paravalvular leaking artificial heart valves and balloon dilatation of narrowed valves.
Structural heart interventions
The Division offers comprehensive evaluation and treatment of most structural heart defects, including atrial septal defect [ASD], patent foramen ovale [PFO], ventricular septal defect [VSD], patent ductus arteriosus [PDA] and interventions on previously operated inborn cardiac defects.?
Infective Endocarditis
The prevalence of infective endocarditis (IE) is very high in South Africa, which is thought to be related to several factors including the high prevalence of valvular heart disease from rheumatic involvement. We prospectively enrolled patients admitted to Tygerberg Academic Hospital (a large academic hospital in the Western Cape province of South Africa serving a population of more than 3 million individuals) to an endocarditis registry (the TEC cohort).
Research from this registry has revealed new trends in causative organisms - including a high rate of Bartonella associated IE and highlighted the importance of a set protocol for organism detection to enable correct therapy. In addition, we have made important recommendations for the early surgical management of high risk patients.
- Pecoraro AJK, Herbst PG, Pienaar C, Taljaard J, Prozesky H, Janson J, Doubell AF. Bartonella species as a cause of culture-negative endocarditis in South Africa. Eur J Clin Microbial Infect Dis. 2021 Apr 7.
https://doi.org/10.1007/s10096-021-04239-w - Pecoraro AJK, Herbst PG, Joubert LH et al. Echocardiographic features of infective endocarditis in South Africa: A prospective cohort study. S Afr Med J 2022; 112(5), 321-327
- Pecoraro AJK, Herbst PH, Pienaar C et al. Modified Duke/ESC 2015 clinical criteria for infective endocarditis: Time for an update? Open Heart 2022 9 (1), e001856.
https://doi.org/10.1136/openhrt-2021-001856 - Pecoraro AJK, Herbst PG, Janson JT et al. Early surgery determines prognosis in patients with infective endocarditis. Cardiovasc Diag Ther 2022; 12 (4) 45.
https://doi.org/10.1086/510583
Peric?ardial disease
The division frequently deals with patients presenting with large pericardial effusions where tuberculous pericarditis is a common cause, but confirming or excluding the diagnosis often depends on cultures that take a long time to yield results. Our group has focused on improving and accelerating the diagnosis of tuberculous pericarditis. Additionally tuberculous pericarditis is frequently complicated by pericardial constriction, a serious complication with high mortality and morbidity. The entity of effusive constrictive pericarditis (ECP) is an important intermediate step between tuberculous pericarditis and the development of pericardial constriction. Although the non-invasive diagnosis of pericardial constriction has been established for some time now, this has not been true for ECP, relying rather on invasive haemodynamics which is particularly problematic in recourses limited settings. Our group has validated the echocardiographic diagnosis of ECP.
- ?Burgess LJ, Reuter H, Carstens ME, Taljaard JJF, Doubell AF. The use of adenosine deaminase and interferon-gamma as diagnostic tools for tuberculous pericarditis. Chest 2002; 122: 900-905. PMID: 12226030.
https://doi.org/10.1378/chest.122.3.900 - ?Van der Bijl P, Herbst PG, Doubell AF. Redefining Effusive-Constrictive Pericarditis with Echocardiography. J Cardiovasc Ultrasound. 2016;24(4):317-323. PMID: 28090260.
https://doi.org/10.4250/jcu.2016.24.4.317
Myoc?arditis
Inflammation of heart muscle (myocarditis) is an important clinical problem that demands a high level of expertise and specialised resources to diagnose and treat. The Division is well-equipped to provide the latest in diagnostic services, including cardiovascular magnetic resonance imaging and heart muscle biopsy when required. Our unit has contributed significantly to the understanding and diagnosis of myocarditis in the largest myocarditis study on the African continent. Not only were much needed data generated from sub-Saharan Africa, but the description of novel biopsy techniques further advanced this field of research.
Related articles:
-
Hassan K, Doubell A, Kyriakakis C, Joubert L, Robbertse PS, Van Zyl G, et al. Comparing the findings and diagnostic sensitivity of cardiovascular magnetic resonance in biopsy confirmed acute myocarditis with infarct-like vs. heart failure presentation. J Cardiovasc Magn Reson. 2022; 24:69.
https://doi.org/10.1186/s12968-022-00903-y -
Hassan K, Kyriakakis C, Doubell A, Van Zyl G, Claassen M, Zaharie D, et al. Prevalence of cardiotropic viruses in adults with clinically suspected myocarditis in South Africa. Open Heart. 2022; 9:e001942.
https://openheart.bmj.com/content/9/1/e001942 -
Hassan K, Kyriakakis C, Joubert L, Van Zyl G, Zaharie D, Doubell A, et al. Routine use of fluoroscopic and real‐time transthoracic echocardiographic guidance to ensure safety of right ventricular endomyocardial biopsy in a low‐volume center. Catheter Cardiovasc Interv. 2022; 99:1563–1571.
https://doi.org/10.1002/ccd.30070 ?
HIV & he?art
The HIV pandemic remains a major health concern and threatens cardiovascular health globally. HIV is especially prevalent in South Africa and other low- to middle income countries. The Division is at the forefront of the study of HIV-associated heart disease, in particular disease of heart muscle (cardiomyopathy). We are proud to have the largest, African research cohort of HIV-infected persons studied over time with cutting-edge diagnostic techniques and making key academic contributions from sub-Saharan Africa.
Related articles:
-
Robbertse PS, Doubell AF, Innes S, Lombard CJ, Herbst PG. Pulse wave velocity demonstrates increased aortic stiffness in newly diagnosed, antiretroviral na?ve HIV infected adults: A case-control study. Medicine. 2022; 101:e29721.
https://doi.org/10.1097%2FMD.0000000000029721 -
Robbertse PS, Doubell AF, Steyn J, Lombard CJ, Talle MA, Herbst PG. Altered cardiac structure and function in newly diagnosed people living with HIV: a prospective cardiovascular magnetic resonance study after the initiation of antiretroviral treatment. Int J Cardiovasc Imaging. 2022; 39:169–182.
https://doi.org/10.1007/s10554-022-02711-y -
Robbertse PS, Doubell AF, Lombard CJ, Talle MA, Herbst PG. Evolution of myocardial oedema and fibrosis in HIV infected persons after the initiation of antiretroviral therapy: a prospective cardiovascular magnetic resonance study. J Cardiovasc Magn Reson. 2022; 24:72.
https://doi.org/10.1186/s12968-022-00901-0 -
Robbertse PS, Doubell AF, Nachega JB, Herbst PG. The hidden continuum of HIV- associated cardiomyopathy?: A focussed review with case reports. SA Heart. 2021; 18:126–135.
http://dx.doi.org/10.24170/18-2-4885 ?
Cardiac Imagin?g
The Division is known locally and internationally as a centre of imaging excellence within both the clinical and research setting. The imaging expertise unit stretches across modalities, including 2D and 3D echocardiography, and state-of-the-art cardiovascular magnetic resonance (CMR) imaging that includes multiparametric mapping.
?CMR cine demonstrations of:

Severe aortic regurgitation
|

Left ventricular hypertrophy in a patient with hypertrophy cardiomyopathy |

Takotsubo cardiomyopathy |
?CMR Images showing:
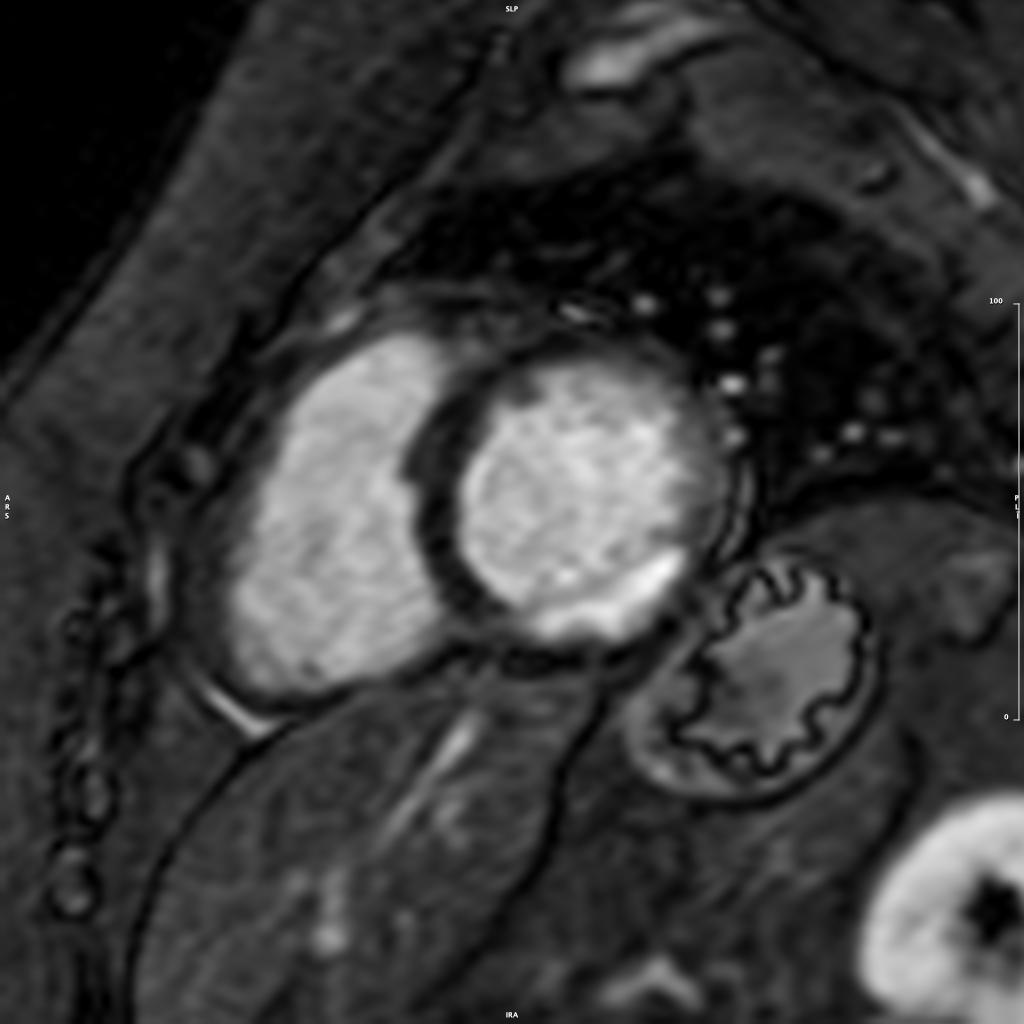
Late gadolinium enhancement
|
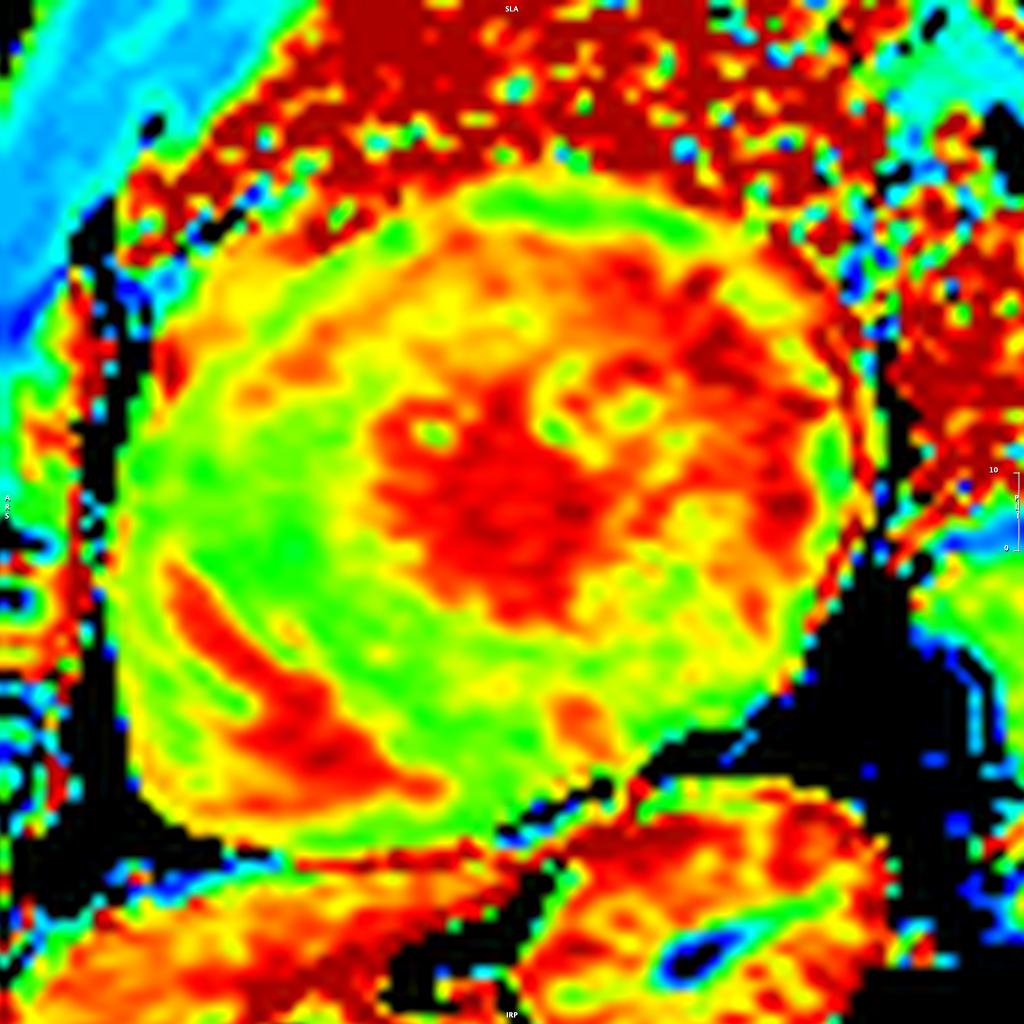
Parametric ECV mapping |
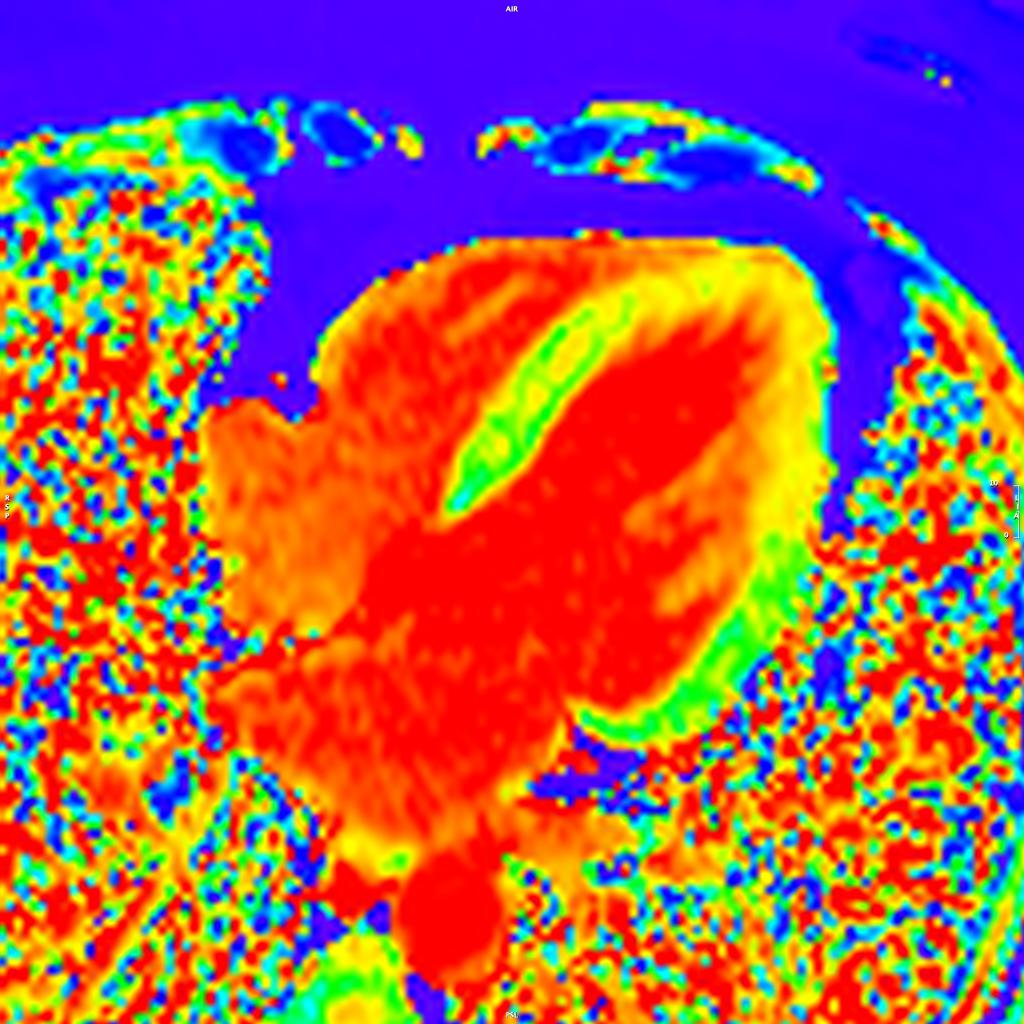
Parametric T1 mapping |
Pulmonary vascular disease
Our division is a national leader in the assessment and treatment of narrowed pulmonary arteries due to previous pulmonary embolism. We are part of a multidisciplinary team specializing in the management of bleeding from the arteries of the lungs [mostly due to TB]
Elec?trophysiology (EP program)
The Division of Cardiology offers both invasive arrhythmia management as well as complex device therapy. The electrophysiology service was launched in 2019. Currently it includes ablation for atrial and ventricular arrhythmias as well as implantation and follow-up of implantable cardioverter-defibrillators, cardiac resynchronisation therapy and conduction system pacing.